Generic
Glomus Jugulare Tumour: Symptoms, Diagnosis & Treatment Options
By Team Hearzap | March 10, 2026
A glomus jugulare tumour is rare, but the symptoms can feel surprisingly familiar, especially if you have a “whooshing” sound in one ear or progressive hearing issues. This guide explains what it is, why it happens, how doctors confirm it, and which treatments are commonly used in India, so you can move from worry to a clear plan.
What is a Glomus Jugulare Tumour?
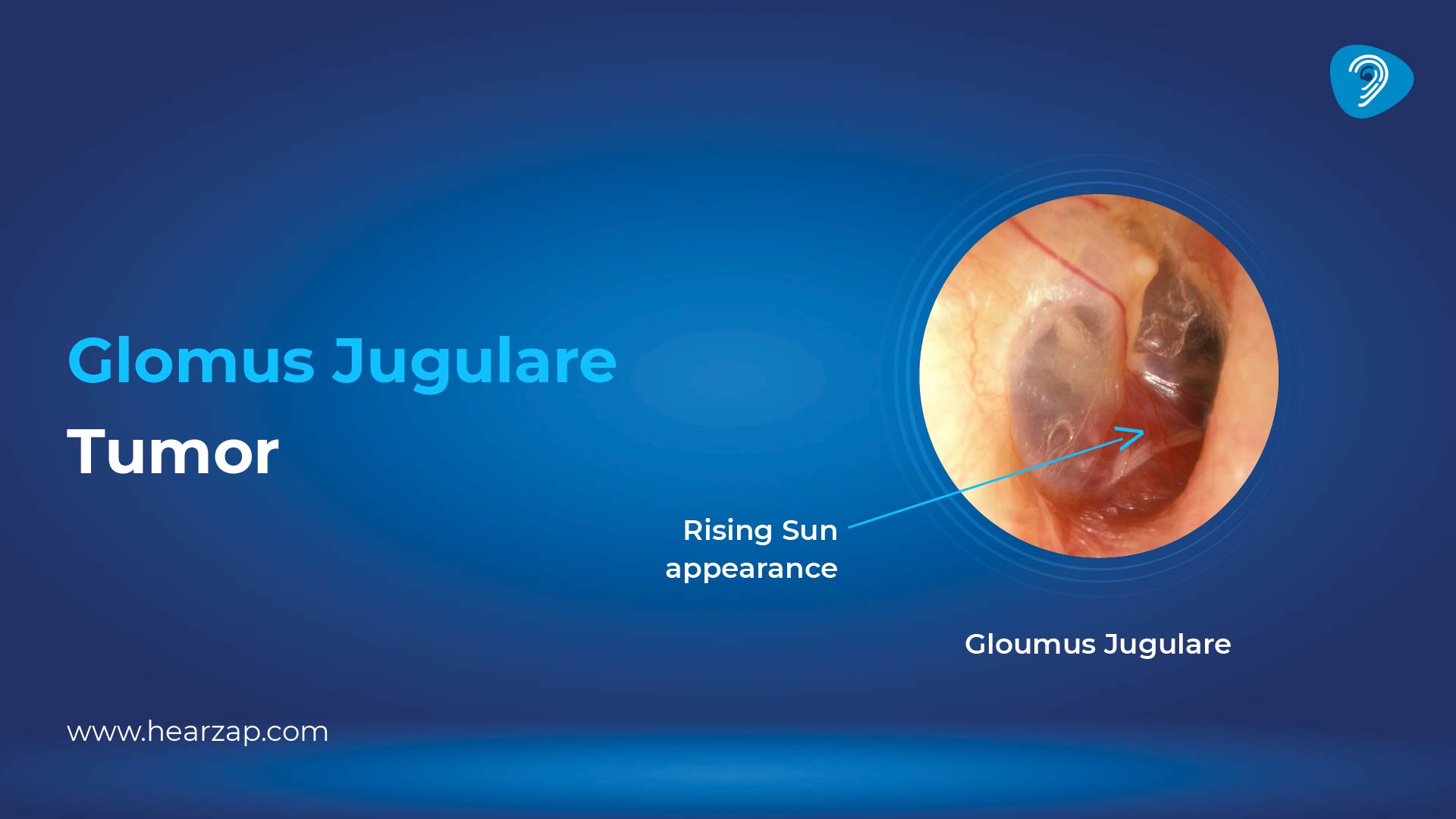
If you’re asking “what is a glomus jugulare tumour?”, think of it as a slow-growing, highly vascular growth that develops near the jugular bulb at the base of the skull. It is a head-and-neck paraganglioma that can affect hearing and nearby cranial nerves, so evaluation and follow-up matter.
Glomus Jugulare Tumour Definition
Glomus jugulare tumour definition: a usually benign paraganglioma arising from paraganglionic cells around the jugular foramen/jugular bulb, characterised by rich blood supply and local spread rather than distant spread.
How Common is Glomus Jugulare Tumour?
These tumours are uncommon. Published estimates put annual incidence around 1–2 per million people, with a clear female predominance reported in health-system reviews. Because they are slow-growing, many people are diagnosed in mid-adulthood after months (or years) of symptoms.
Glomus Jugulare Tumour Symptoms
Most symptoms come from two factors: sound/vibration from the tumour’s blood flow, and pressure on nearby structures. The pattern often starts subtly and then becomes more specific as the growth enlarges.
Early Symptoms
Common early glomus jugulare tumour symptoms include:
- Pulsatile tinnitus (a heartbeat-like “whoosh” in one ear)
- Gradual hearing loss (often conductive at first)
- A feeling of fullness in the ear
- Occasional ear pain or discharge (less common)
If hearing feels reduced, an online hearing test can be a useful first screen, but it cannot identify the cause. Persistent one-sided symptoms still need an in-person ear examination.
For some people, addressing hearing impact early, such as choosing to buy hearing aids online after a proper evaluation, can improve day-to-day comfort while the tumour work-up and treatment plan are being finalised.
Advanced Symptoms
As the tumour grows, symptoms may reflect involvement of cranial nerves at the skull base. Possible advanced features include:
- Hoarseness or voice change
- Swallowing difficulty (dysphagia) or choking episodes
- Weakness of facial muscles or asymmetry
- Tongue weakness, shoulder droop, or reduced gag reflex
- Persistent dizziness or balance problems
These signs are more urgent because they can indicate skull-base nerve involvement.
Causes and Risk Factors
This tumour forms from paraganglionic tissue (cells linked to nerve pathways that can act as chemoreceptors). Most are sporadic, but a meaningful minority are linked to inherited tumour syndromes, which is why family history and genetic assessment may be suggested.
Genetic Associations
Genes related to the succinate dehydrogenase (SDH) complex are the best-known inherited links. Pathogenic variants, especially SDHD and SDHB, can increase the likelihood of head-and-neck paragangliomas, and they may raise the chance of multifocal disease, so long-term surveillance is sometimes advised.
Risk doesn’t mean certainty. Many people with this tumour have no family history, and many families with SDH variants never develop this specific skull-base growth.
Glomus Jugulare Tumour Diagnosis
Diagnosis usually relies on examination and imaging, as these tumours are highly vascular. In practice, the aim is to confirm location, map blood supply, and define nerve and bone involvement – this is the core of glomus jugulare tumour radiology, and it guides treatment choice.
Doctors start with otoscopy, a hearing assessment, and cranial nerve checks. If hormone-related symptoms occur, blood and urine tests may be advised.
Imaging Tests (Radiology)
Doctors commonly use a combination of:
- Contrast MRI to evaluate soft tissue spread and intracranial extension; classic lesions can show a “salt-and-pepper” appearance from flow voids
- High-resolution CT (temporal bone/skull base) to assess bone erosion and jugular foramen enlargement
- Angiography (digital subtraction angiography) when detailed vessel mapping is needed, often for surgical planning or pre-operative embolisation
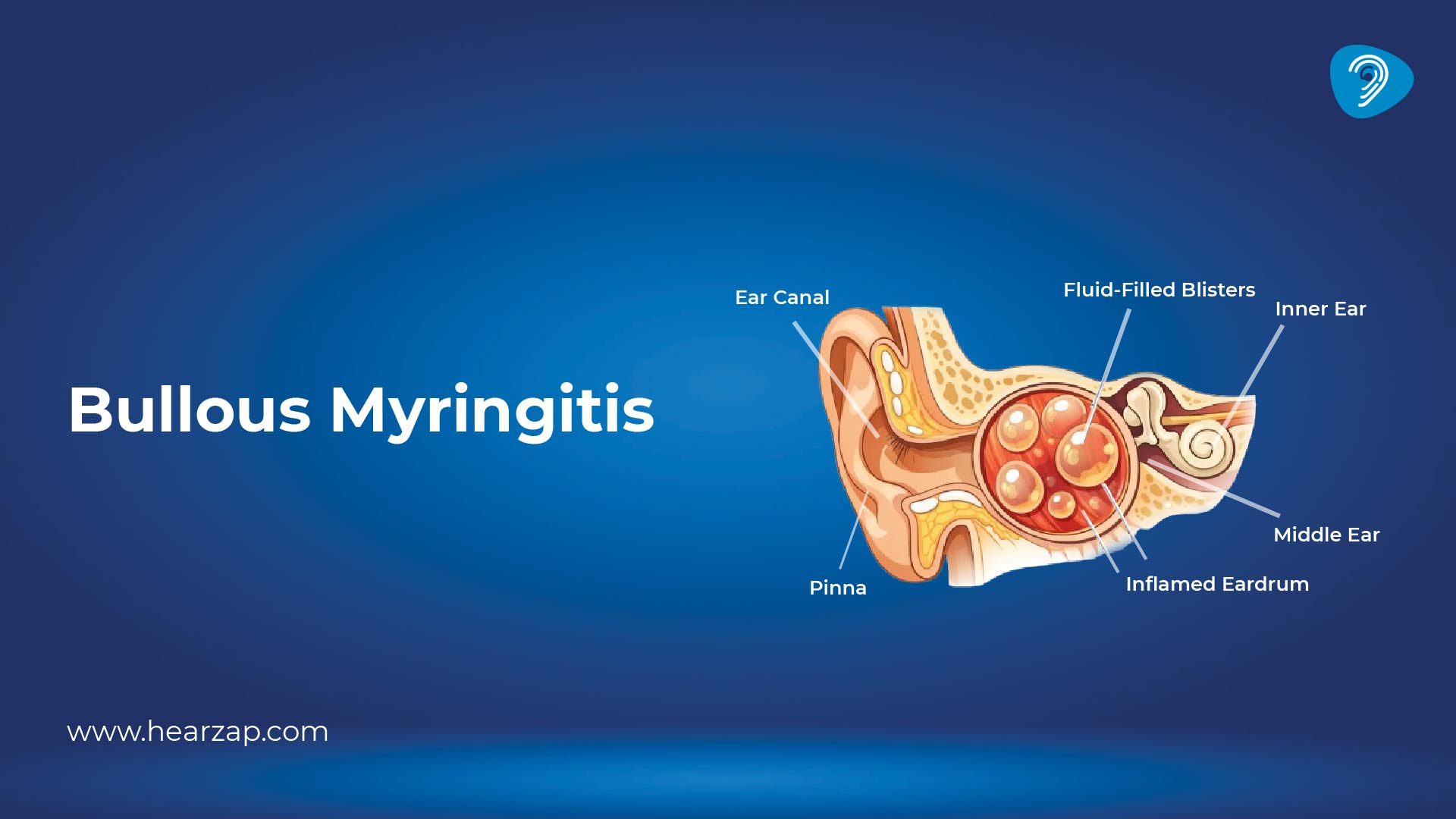
Imaging can also help distinguish a vascular mass from other causes of ear symptoms, such as bullous myringitis, which is inflammatory and typically presents very differently on examination.
Biopsy and Pathology
Because these tumours are so vascular, biopsy is not routinely the first step and is usually avoided unless a specialist team believes it is necessary and safe. When tissue is obtained (often during treatment), pathology confirms a paraganglioma pattern and helps assess features linked to behaviour and follow-up needs; this is where glomus jugulare tumour pathology outlines become medically meaningful for your care plan.
It’s also important to rule out common “look-alikes” in the ear. For example, scarring of the eardrum (Tympanosclerosis) can affect hearing but does not produce the vascular imaging signature seen with glomus tumours.
Treatment of Glomus Jugulare Tumour
Treatment of glomus jugulare tumour is personalised. Doctors weigh tumour size, growth rate, hearing status, cranial nerve function, age, pregnancy plans, and overall health. In many centres, a multidisciplinary team (ENT skull-base surgeon, neurosurgeon, interventional radiologist, and radiation oncologist) jointly plans care.
Glomus Jugulare Tumour Surgery
Glomus jugulare tumour surgery aims to remove as much tumour as safely possible, relieve pressure effects, and prevent future progression. Surgery can be curative for selected tumours, but it is technically demanding due to the blood supply and proximity to cranial nerves.
Potential benefits:
- Immediate tumour debulking/removal
- Tissue diagnosis and grading
- Symptom improvement in carefully selected cases
Potential risks (discussed in detail before surgery):
- Cranial nerve deficits affecting voice or swallowing
- Hearing changes
- Bleeding (sometimes reduced with pre-operative embolisation)
- Need for rehabilitation, speech/swallow therapy, or staged treatment
Your surgeon will also explain scar planning, as the incision location varies depending on the approach.
Radiation Therapy
Radiotherapy, including stereotactic radiosurgery, is widely used for tumour control, especially when surgery risks high morbidity or when residual tumour remains after partial removal. Many modern series report good local control with lower nerve-related complications than with extensive skull-base resection, although long-term follow-up is limited.
Radiation is not “instant.” The goal is typically to stop growth, and shrinkage may be slow, so symptom monitoring stays important.
Observation (Wait and Watch)
Because many of these tumours grow slowly, observation is a valid option for small, minimally symptomatic tumours, older patients, or those with higher operative risk. This approach relies on periodic MRI and hearing assessment, plus prompt review if symptoms change.
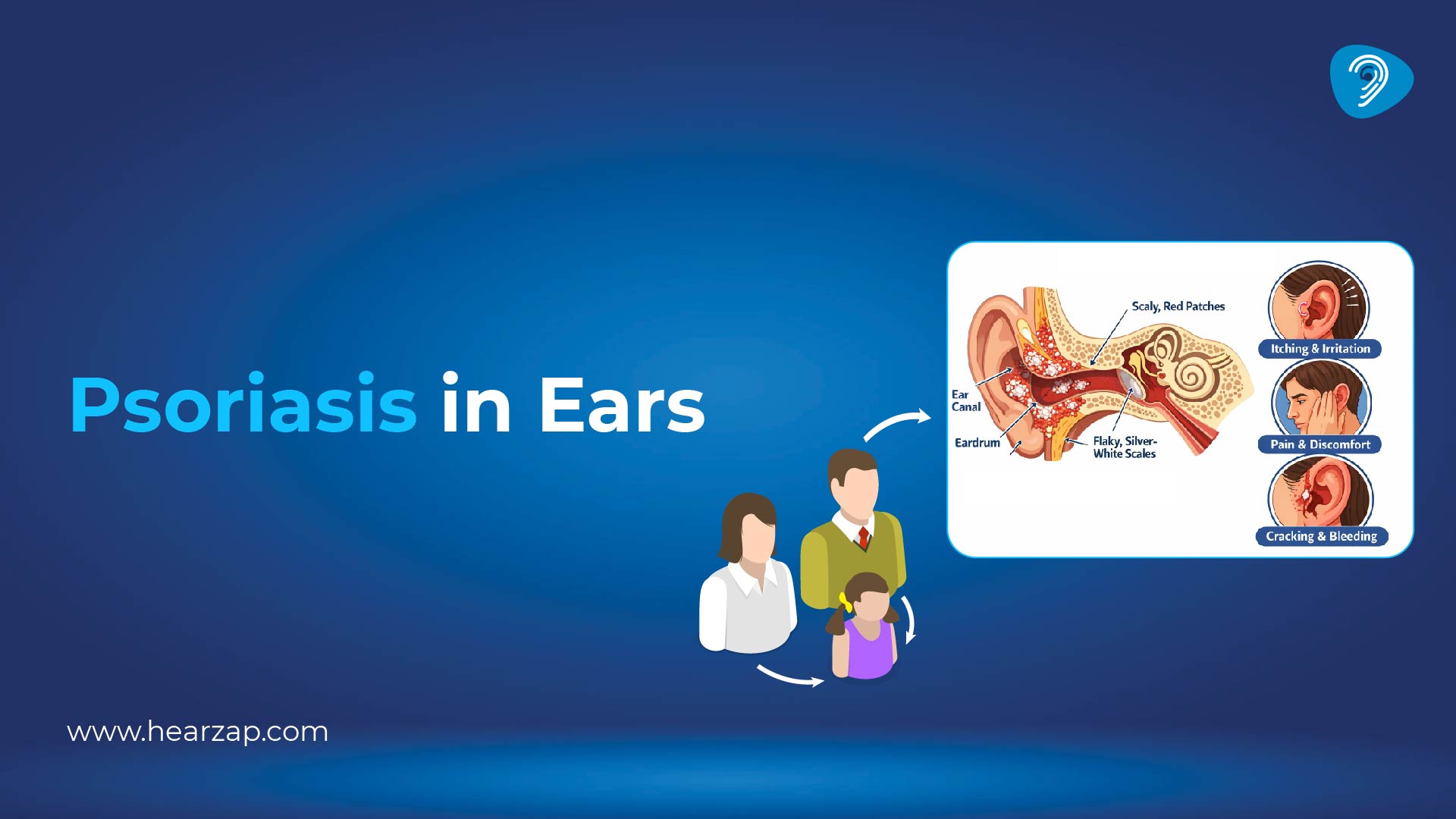
During observation, doctors also consider other ear problems that can mimic symptoms. For instance, itching and scaling from psoriasis in ear can cause discomfort and blockage sensations, but it needs a different treatment pathway.
Recovery and Scar After Surgery
Recovery depends on tumour size, approach, and whether nerves were involved before treatment. In the first few weeks, fatigue, ear fullness, and temporary swallowing discomfort are common, and you may need a soft diet or voice rest.
When people search scar glomus jugulare tumour, they are usually worried about where the cut will be and whether it shows. Most skull-base approaches place the incision behind the ear and into the neck crease, so it can be hidden by the hairline and natural skin folds. If there is an ear scar glomus jugulare tumour concern, ask your surgeon to show you the planned incision line, discuss scar care (silicone gel, sun protection), and clarify when you can safely resume hair colouring or salon treatments.
Glomus Jugulare Tumour Prognosis
Prognosis is often favourable because these tumours are typically benign and slow-growing, though they can be locally aggressive. Metastasis is uncommon in most reviews, but long-term follow-up is important because recurrence or regrowth can occur, especially after subtotal resection or in hereditary disease. Control rates are generally high with modern surgery and/or radiotherapy, and many people live normal lifespans with monitoring.
When to See a Doctor
Seek medical care if you have:
- Pulsatile tinnitus in one ear, especially if persistent
- Progressive one-sided hearing loss or new imbalance
- A visible reddish mass behind the eardrum on examination
- Hoarseness, swallowing difficulty, facial weakness, or tongue/shoulder weakness
If symptoms are sudden, severe, or paired with neurological changes, treat it as urgent.
FAQs
What is the triad of glomus tumour?
In everyday teaching, the common triad described for middle-ear paragangliomas is pulsatile tinnitus, hearing loss, and a vascular-looking mass behind the eardrum on examination. Not every person has all three, and skull-base involvement may add nerve-related symptoms.
How long is recovery for glomus tumour removal?
Many people need several weeks to feel “back to normal”, but recovery varies widely. Minor tumours may allow earlier return to desk work, while larger skull-base operations can require longer healing and rehabilitation, especially if swallowing or voice therapy is needed.
Is this tumour cancerous?
Most are benign, meaning they do not behave like typical cancers that spread widely. However, they can be locally invasive, and a small minority can metastasise, so follow-up imaging matters.
Which specialist should you consult in India?
Start with an ENT specialist (otology/skull base). If a glomus jugulare tumour is suspected, you are usually referred to a skull-base team that includes neurosurgery and radiation specialists for a combined plan.
Can symptoms come back after treatment?
They can. Regrowth or recurrence is more likely when complete removal is not safe or when there is a hereditary risk. Regular follow-up appointments and imaging help catch changes early.

Contact us
We are here for all your hearing needs, from hearing tests to hearing aids. Fill out the form below, and we will give you a call soon.
Recent Blogs
By None | March 11, 2026
By None | March 9, 2026
By None | March 7, 2026
By None | March 6, 2026
By Team Hearzap | March 4, 2026









