Generic
Glomus Tympanicum: A Rare Ear Tumor You Should Know About
By Team Hearzap | March 30, 2026
Have you ever heard your own heartbeat thumping inside your ear constantly like a drum you can't turn off? Most people assume it's nothing. Maybe stress. Maybe tiredness. They wait it out, and it doesn't go away.
For a small number of people, that sound has a name. And knowing what it is changes everything.
What Is a Glomus Tympanicum?
Inside your body, scattered in various places, are tiny structures called glomus bodies. They're minuscule clusters of blood vessels and nerve cells that help regulate blood flow. You'd never know they were there.
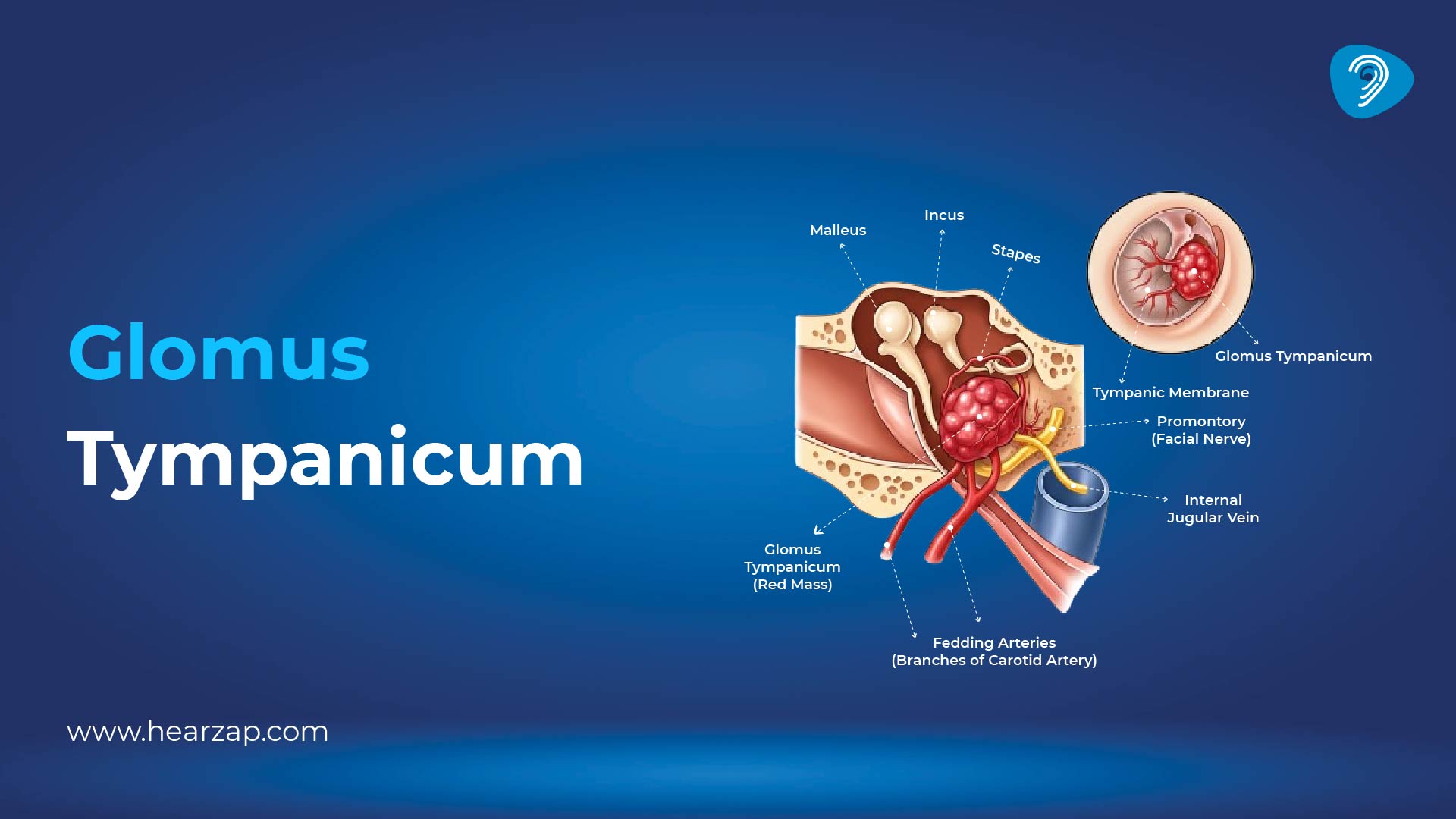
But occasionally, the cells in one of these structures start growing when they shouldn't. They form a small tumor. When this happens inside the middle ear (small air-filled space just behind your eardrum), it's called a glomus tympanicum tumor.
These tumors are almost always benign. They don't spread. They grow slowly. In many ways, they're more of a structural nuisance than a medical emergency. But because they're growing in an incredibly small, sensitive space right next to your eardrum, your hearing bones, and major blood vessels, even a tiny growth makes its presence known.
They're more common in women, tend to appear between the ages of 40 and 70, and are the most common benign tumor of the middle ear. That said, they're still rare. Most medical professionalsl only encounter a handful of cases in their entire career.
What Does It Actually Feel Like?
This is where glomus tympanicum has a very particular signature.
The standout symptom is pulsatile tinnitus, a rhythmic, whooshing or thumping sound in the ear that beats in time with your own pulse. Not a constant ring. Not static. A pulse. Some people describe it as hearing their heartbeat inside their head. Others say it sounds like a distant drum. It's relentless, and it's almost impossible to ignore once it starts.
Pressing on a vein in the neck or changing head position can sometimes briefly change or muffle the sound — which is actually a clue doctors use when trying to figure out what's causing it.
Alongside the noise, many people notice hearing loss in the affected ear. The tumor sits right next to the tiny bones that conduct sound, and even a small growth pressing against them can dull hearing noticeably.
If a doctor peers into the ear with an otoscope, they may spot something unusual: a reddish or reddish-blue bulge behind the eardrum, sometimes visibly pulsating. It looks a little startling when you see it for the first time, but it's actually one of the clearest diagnostic clues there is.
Some patients also feel a sense of fullness or pressure in the ear. In more advanced cases, dizziness can creep in, or — if the tumor has grown enough to press on the facial nerve — a slight weakness on one side of the face.
Glomus Tympanicum Classification: How Doctors Size It Up
Once a tumor like this is identified, doctors need to understand exactly how far it's grown. That's where the glomus tympanicum classification system comes in — specifically the Fisch classification, which divides tumors into four types based on size and spread.
Type A is the earliest stage. The tumor is small and sitting neatly in the middle ear, along the nerve pathway on the eardrum's inner surface. Straightforward to treat, excellent outcomes.
Type B has grown a little further into the middle ear cavity but hasn't started eating into the bone beneath it. Still very manageable.
Type C is where things get more serious. The tumor has begun to invade the bone at the base of the skull and is creeping toward the passage carrying the main artery to the brain. More complex surgery is needed.
Type D has extended into the skull itself. Rare, and requires highly specialised surgical teams.
The good news is that most people are diagnosed at Type A or B — when the tumor is still contained and treatment is highly effective.
Glomus Tympanicum Radiology: Looking Through Bone
You can't examine the middle ear with a standard check-up. The whole thing is enclosed in some of the densest bone in the human body. So imaging — glomus tympanicum radiology — is what allows doctors to actually see what's going on.
A CT scan is usually the first step. It gives a crisp, detailed picture of all the bony structures of the ear. In a glomus tympanicum, the CT typically shows a small soft-tissue mass sitting on the inner wall of the middle ear — and crucially, the surrounding bone looks intact. No erosion. That matters, as you'll see in a moment.
MRI adds another layer of detail, showing how the tumor relates to surrounding soft tissue and blood vessels. On MRI, these tumors have a distinctive appearance — radiologists describe it as "salt and pepper," a mix of bright and dark patches caused by the constant, rapid blood flow moving through the tumor's dense network of tiny vessels.
In larger tumors, doctors may also use angiography — an imaging technique that maps blood vessels using dye — to plan surgery or to cut off the tumor's blood supply beforehand, reducing the risk of heavy bleeding during removal.
Glomus Jugulare vs Tympanicum Radiology: Getting the Diagnosis Right
Here's where it gets a little more nuanced — and where getting the right answer really matters.
There's a closely related tumor called the glomus jugulare. Both are glomus tumors near the ear, both cause that same pulsating heartbeat sound, and both can look similar on imaging at first glance. But they are not the same thing, and distinguishing glomus jugulare vs tympanicum radiology is one of the most important steps in the diagnostic process.
A glomus jugulare starts lower down — at the jugular bulb, a widening of the large vein that drains blood from the brain, sitting just beneath the middle ear at the base of the skull. From there, it tends to grow upward into the middle ear and downward into the neck. It's typically larger, more invasive, and far more complex to treat.
The clearest difference on imaging? Bone destruction. A glomus jugulare characteristically erodes the bone around the jugular foramen — that opening at the skull base through which the vein passes. On CT, this creates a distinctive "moth-eaten" appearance that you simply don't see with a glomus tympanicum, which tends to sit politely in the middle ear without chewing through bone.
On MRI, both tumors show that same "salt and pepper" pattern, so location — not appearance — is what separates them. The glomus tympanicum originates from the middle ear wall. The glomus jugulare originates from below. That distinction shapes everything that follows, because the surgical approach, the team required, and the risks involved are entirely different.
Treatment: What Are the Options?
For most people with a Type A or B tumor, surgery is the recommended route — and it works well. The tumor is accessed through the ear canal or behind the ear, removed under general anaesthetic, and in experienced surgical hands, the success rate is high. Recurrence is uncommon. Many patients notice their pulsatile tinnitus disappears almost immediately after the tumor is removed.
For those who would rather avoid surgery — or for whom surgery carries higher risks due to age or health — stereotactic radiosurgery (often called Gamma Knife) is a well-established alternative. This isn't traditional radiation therapy. It's a single, precisely targeted treatment that uses focused beams to stop the tumor growing, without an incision. It controls the tumor effectively in most cases, though the thumping sound in the ear may linger even after treatment.
For elderly patients with very small, slow-growing tumors and mild symptoms, active monitoring — regular imaging with no immediate intervention — is sometimes the most sensible path. These tumors grow so slowly that the risks of treatment may outweigh the benefits in certain situations.
The Bottom Line
A tumor in the ear sounds frightening. Understandably so. But a glomus tympanicum, in most cases, is about as treatable as it gets. It's slow, it's contained, it rarely causes serious harm, and when it's caught and managed early, people do very well.
The thing that tends to delay diagnosis isn't the complexity of the condition — it's that rhythmic heartbeat in the ear being dismissed as anxiety, or ignored for years until something prompts a proper look. If you or someone you know has been living with a pulsing sound in one ear that beats with the heart, that symptom alone is worth taking to a doctor. It's a specific enough clue that the right specialist will know exactly what to look for.
FAQs
What is a glomus tympanicum?
A rare, usually benign tumor that forms in the middle ear from paraganglionic cells.
What is the difference between glomus tympanicum and paraganglioma?
Glomus tympanicum is a type of paraganglioma specifically located in the middle ear.
How do you treat glomus tympanicum tumor?
Treatment typically includes surgical removal, sometimes combined with radiation therapy.
What is the triad of glomus tumor?
The classic triad includes pulsatile tinnitus, hearing loss, and a visible reddish mass behind the eardrum.

Contact us
We are here for all your hearing needs, from hearing tests to hearing aids. Fill out the form below, and we will give you a call soon.
Recent Blogs
By Team Hearzap | March 27, 2026
By None | March 26, 2026
By None | March 25, 2026
By None | March 23, 2026
By None | March 18, 2026









