HEARING CARE
Otosclerosis: When Your Ear's Own Bone Works Against You
By Team Hearzap | May 13, 2026
Most people, when they think about hearing loss, picture the inner ear gradually wearing out. Overexposure to noise. Ageing. Maybe genetics catching up with you. What very few people consider is that the problem might be structural. Mechanical. A tiny bone in the middle ear that has essentially seized up and stopped doing its job.
That's otosclerosis. And for the people living with it, often for years before getting a proper diagnosis, understanding what's actually happening inside the ear changes everything.
What Is Otosclerosis?
Before getting into the condition itself, a tiny bit of anatomy is genuinely helpful here.
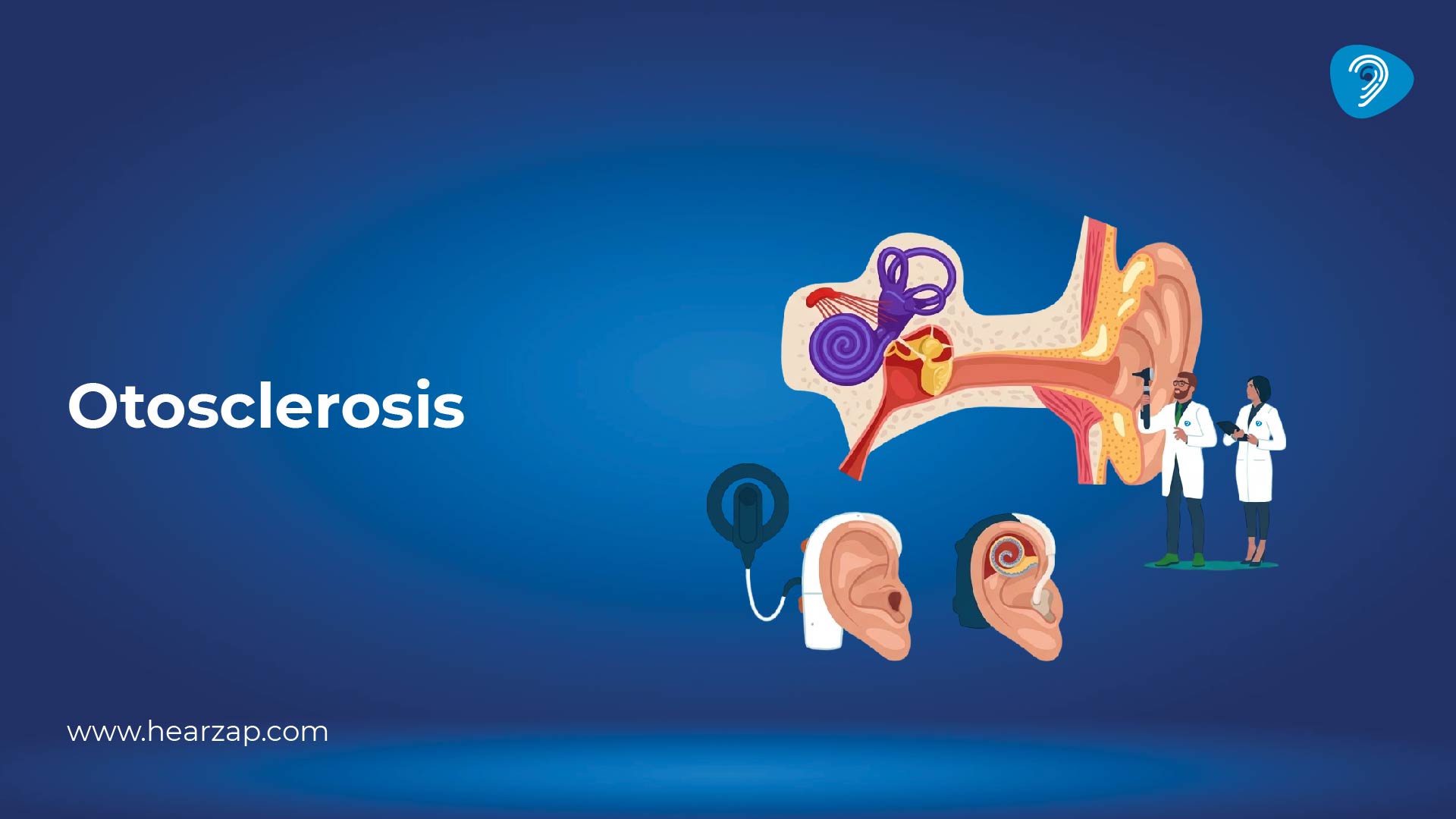
Inside your middle ear sit three of the smallest bones in the human body. They're called the malleus, the incus, and the stapes, and together they form a miniature chain that carries sound vibrations from your eardrum into your inner ear. The last bone in that chain, the stapes, sits in a tiny opening called the oval window. When sound arrives, the stapes vibrates like a piston, pushing those vibrations into the fluid of the cochlea, which then converts them into signals your brain reads as sound.
What is otosclerosis in this context? It's what happens when abnormal bone growth forms around the stapes and that oval window. This new bone is irregular and spongy, and over time it locks the stapes in place. A bone that's supposed to vibrate hundreds of times a second simply can't move anymore. Sound transmission breaks down. Hearing loss follows, slowly but steadily.
The otosclerosis definition used in clinical medicine describes it as a pathological remodelling of the bony labyrinth of the inner ear, leading to progressive fixation of the stapes. Translated into plain language: the ear starts growing bone in places it shouldn't, and the consequences creep up on you over years.
Who Tends to Get It?
Otosclerosis has a few consistent patterns worth knowing about.
It runs in families. There's a clear genetic component, though having the gene doesn't automatically mean you'll develop the condition. Environmental triggers, including a past measles infection and hormonal shifts, particularly oestrogen, seem to influence whether the gene actually activates. This is thought to be one reason why pregnancy can accelerate progression in some women.
It affects women more often than men. It typically appears somewhere between the ages of 15 and 45, making it unusual among hearing conditions in that it often strikes relatively young, otherwise healthy adults. It most commonly affects both ears eventually, though one side usually becomes noticeable before the other. And it is more prevalent in white and South Asian populations than in others.
Otosclerosis Symptoms: What It Actually Feels Like
This is where things get frustrating for a lot of patients, because otosclerosis symptoms arrive so gradually that they're easy to dismiss for a long time.
The earliest sign is usually difficulty following conversations when there's background noise. You start turning up the television slightly. You ask people to repeat themselves more than you used to. It doesn't feel dramatic at first. It just feels like you're not quite catching everything.
As things progress, the picture becomes clearer:
- Progressive hearing loss that worsens over months and years, starting in one ear and eventually affecting both
- Tinnitus, a persistent ringing, hissing, or buzzing sound in the ear, which many patients find particularly wearing
- Paracusis Willisii, a curious phenomenon where hearing actually seems better in noisy places. This sounds strange, but it happens because background noise prompts people to speak louder, which genuinely helps those with conductive hearing loss hear more clearly
- A sense of muffled hearing, as though someone has turned the volume down and partially blocked the speaker
- Dizziness or balance issues in a smaller subset of patients, particularly when the inner ear becomes more involved over time
Because the changes are gradual and one ear often compensates for the other initially, people frequently adapt without realising how much hearing they've actually lost. Many patients look back and say they'd been struggling for five or ten years before they finally sought help.
Otosclerosis Audiogram: Reading the Clues
When someone comes in with this pattern of hearing loss, a detailed hearing assessment is the first proper investigative step. The otosclerosis audiogram has some fairly distinctive features that point clearly toward the diagnosis.
The classic finding is something called a Carhart notch, a characteristic dip in bone conduction thresholds at around 2000 Hz. This isn't a true inner ear problem. It's a mechanical effect of the stapes being fixed, showing up on the hearing test as a false sensorineural loss. Alongside this, the overall audiogram typically shows a conductive pattern, where air conduction scores are significantly worse than bone conduction scores. This tells the audiologist that the inner ear itself is largely intact but the mechanical transmission of sound through the middle ear bones is impaired.
Tympanometry, a quick additional test that measures eardrum and middle ear movement, often shows a shallow, flat pattern called an A curve, reflecting the reduced mobility of the ossicular chain. Together, these findings build a fairly clear picture.
Otosclerosis Radiology: When Imaging Adds to the Story
Imaging isn't always necessary for a straightforward diagnosis, but otosclerosis radiology becomes important when the picture is less clear or when surgery is being planned.
High resolution CT scanning of the temporal bone is the gold standard. On CT, otosclerosis typically shows up as areas of decreased bone density around the oval window and the cochlear capsule. In more advanced cases, there may be a visible halo of abnormal bone surrounding the cochlea, sometimes called the double ring sign. This not only confirms the diagnosis but also helps the surgeon understand how far the abnormal bone growth has spread before they operate.
MRI is occasionally used when there's concern about inner ear involvement, but CT remains the first choice for most cases.
Otosclerosis Treatment: The Options on the Table
Otosclerosis treatment is, genuinely, one of the better news stories in ear medicine. Most patients have real options, and the outcomes are often excellent.
- Hearing aids work very well for early otosclerosis because the inner ear is usually still healthy. Good amplification compensates effectively for the conductive loss. For patients who aren't ready for surgery, or who have other health factors that make surgery inadvisable, a well-fitted hearing aid can restore functional hearing to a high standard.
- Sodium fluoride has historically been used to try to slow the abnormal bone growth. The evidence is mixed, and it's not widely used today, but it remains an option in specific circumstances, particularly for patients with active progression who aren't surgical candidates.
- Surgery is the definitive treatment for most people, and it works remarkably well. The procedure is called a stapedectomy or stapedotomy. The surgeon accesses the middle ear through the ear canal, removes the fixed stapes bone, and replaces it with a tiny prosthesis, usually a titanium piston, that restores the movement the natural bone has lost.
Otosclerosis surgery has a high success rate. The large majority of patients experience significant hearing improvement, with many returning to near-normal levels. It's typically a day procedure, performed under general or local anaesthetic, and takes roughly 90 minutes. Some dizziness and mild discomfort in the first few days is expected as the ear settles, but this usually resolves quickly.
As with any surgery, risks exist. There's a small chance of tinnitus worsening, incomplete improvement, or in rare cases, further hearing loss in the operated ear. These risks are real and any good surgeon will discuss them honestly before proceeding. But for most healthy, suitable patients, the risk-benefit balance sits clearly in favour of surgery.
The Bottom Line
Otosclerosis is one of those conditions that hides in plain sight. It progresses slowly, it's easy to rationalise away, and it's often missed for years because patients and sometimes doctors aren't thinking about a structural middle ear problem in a thirty-five year old.
But it has a recognisable fingerprint on a hearing test, a visible pattern on imaging, and treatments that genuinely restore hearing rather than just managing decline. If you're in your twenties, thirties, or forties and your hearing has been quietly getting worse without explanation, it's worth raising this specifically with your doctor. The answer might be sitting in a tiny bone you never knew existed.
FAQs
Why Carhart notch in otosclerosis?
Carhart notch occurs due to stapes fixation affecting bone conduction, especially around 2000 Hz.
Can otosclerosis be cured?
Otosclerosis cannot be fully cured but can be effectively treated with surgery or hearing aids.
What causes otosclerosis?
Otosclerosis is caused by abnormal bone growth in the middle ear, often linked to genetic factors.
Can otosclerosis cause headaches?
Otosclerosis does not typically cause headaches but may cause ear-related discomfort.
Is otosclerosis unilateral or bilateral?
Otosclerosis is usually bilateral but may start in one ear first.
Related Blogs

Auditory Neuropathy Spectrum Disorder

Vestibular Migraine: When Dizziness Is the Headache
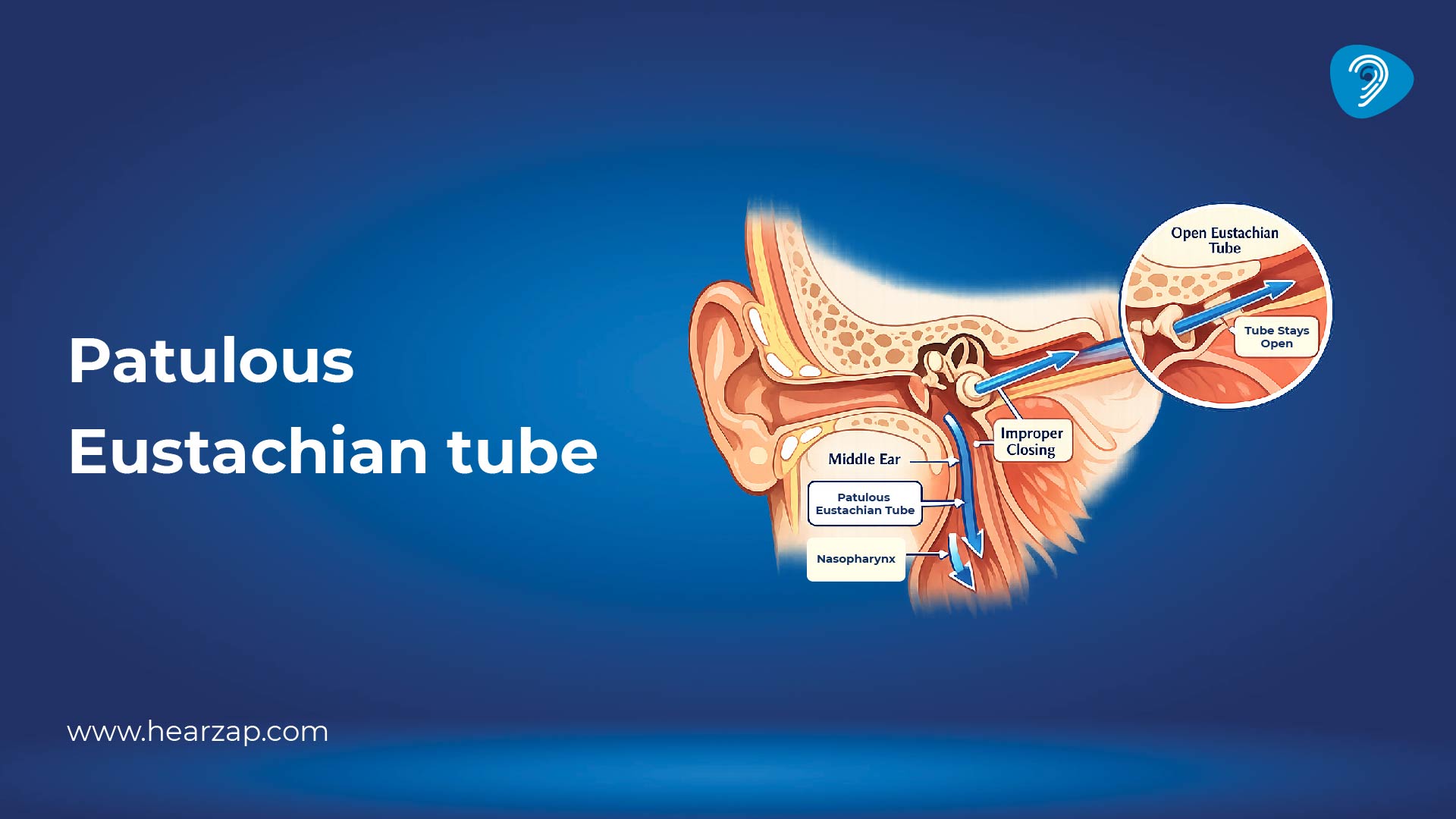
Patulous Eustachian Tube
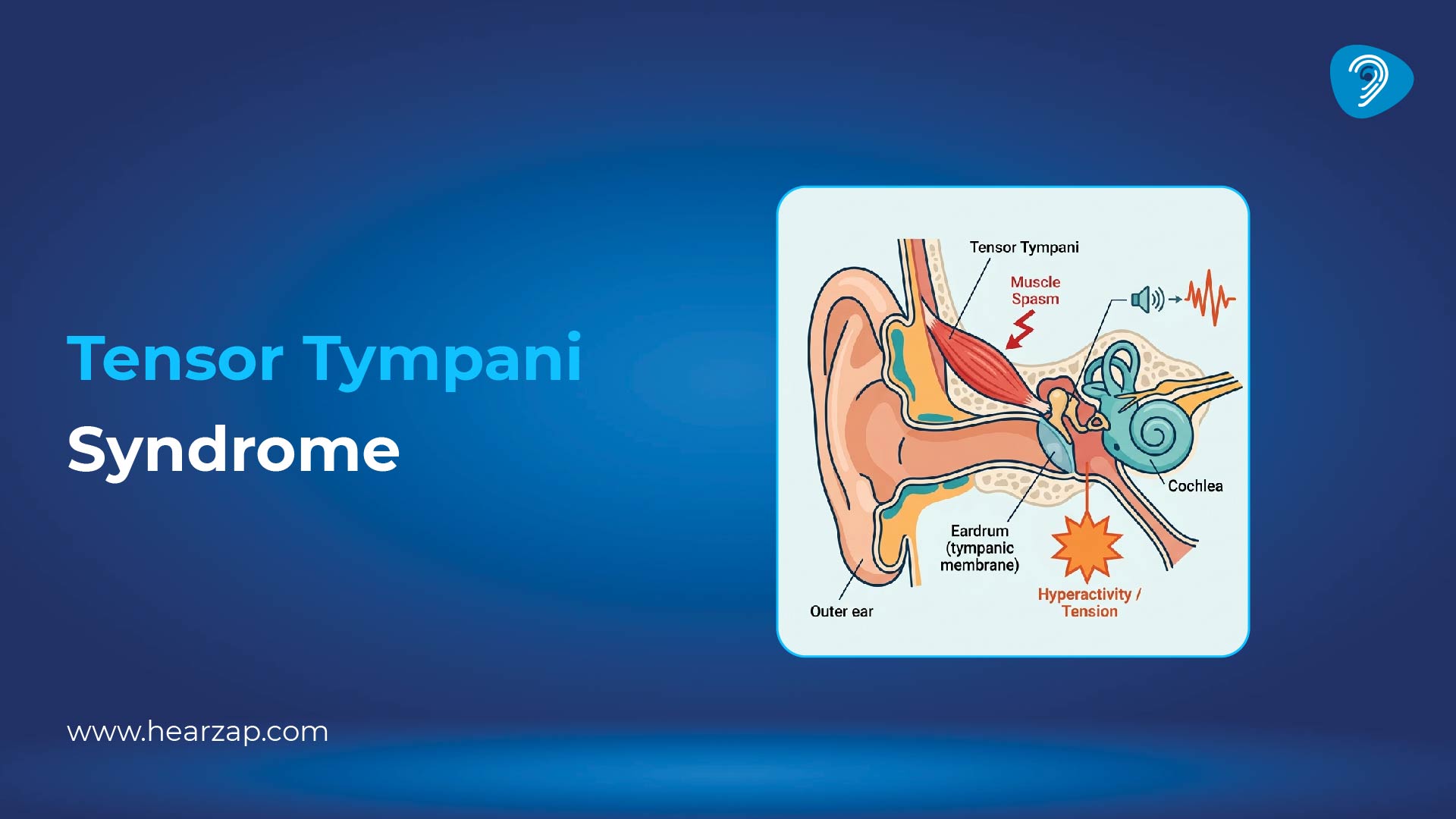
Tensor Tympani Syndrome
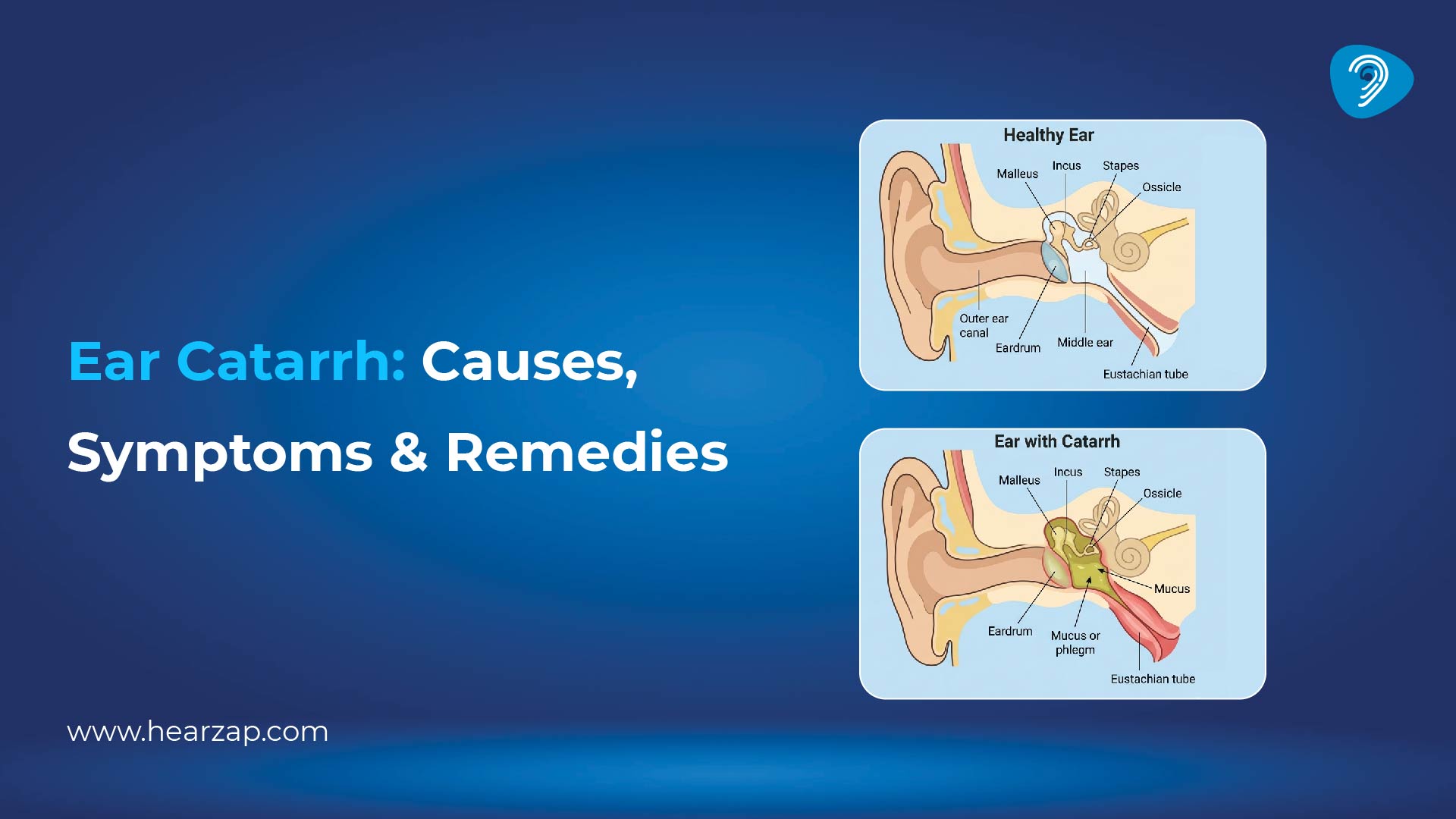
Ear Catarrh: Causes, Symptoms, Treatment & Home Remedies

Hyperacusis: Causes of Hearing Sensitivity and Treatment Options
Seborrheic Dermatitis in the Ear
Contact us
We are here for all your hearing needs, from hearing tests to hearing aids. Fill out the form below, and we will give you a call soon.
Recent Blogs
By Team Hearzap | July 4, 2026
By Team Hearzap | July 3, 2026
By Team Hearzap | July 2, 2026
By None | July 1, 2026
By None | June 25, 2026









